 The following paper was originally presented by SSI Senior Associate Peter Diamandis at the 1987 SSI/AIAA/Princeton Space Manufacturing Conference.
The following paper was originally presented by SSI Senior Associate Peter Diamandis at the 1987 SSI/AIAA/Princeton Space Manufacturing Conference.
It has been highly cited over the years in many later discussions and reviews of Artificial Gravity concepts, but for new researchers it has been difficult to acquire as Peter retained his copyright and thus it could only be found in the printed edition of the SSI/AIAA “Space Manufacturing volume 6: Nonterrestrial Resources, Biosciences and Space Engineering”
The Space Studies Institute thanks Peter for recently giving SSI the rights to provide this excellent, in depth yet highly readable paper to a new generation of Artificial Gravity researchers.
The SSI G-Lab is not a simple project but it is incredibly important and by knowing all the facts We Can make it happen the right way. Thank you for your support!
RECONSIDERING ARTIFICIAL GRAVITY FOR TWENTY-FIRST CENTURY SPACE HABITATS
Peter H. Diamandis*
Massachusetts Institute of Technology
Harvard Medical School
* Peter H. Diamandis is a MD-PhD candidate at HMS and MIT. His research is conducted at M.I.T.’s Man-Vehicle Laboratory.
Abstract:
The paper examines the medical rationale for artificial gravity and reviews past investigations into the optimal rotation velocity and habitat radius. The paper also proposes new directions for research in the field of Artificial Gravity.
1. INTRODUCTION
When humans first entered space, physicians, scientists and engineers made widely varying predictions of how the body would react to zero gravity. Some hypothesized an inability to swallow without gravity and others predicted that a total cardiovascular collapse would occur. Today, a quarter century later, we are just beginning to understand the medical and human factors side of living and working in microgravity, and it is at this time appropriate to seriously address the following questions surrounding the concept of artificial gravity.
- Why should we consider Artificial Gravity?
- How much Artificial Gravity is needed?
- When is Artificial Gravity inappropriate?
- What are the physiologic limits to radius and angular velocity?
- What are the cost limits to radius and angular velocity?
Why do we need Artificial Gravity in orbiting habitats? Twenty years ago the answer would have been given by the human factors and space manufacturing groups — in particular, that artificial gravity is necessary to allow astronauts to properly handle materials, complete manual tasks, and maneuver easily about the space craft. Today however, after numerous experiences on Skylab, Spacelab and the Space Shuttle, we realize that gravity is not needed for work or construction in space, nor is it necessary for the run-of-the-mill activities aboard the spacecraft.
Today the answer as to why we might need artificial gravity is given by the physicians. Medical research on the long term medical effects of microgravity indicate that our major concern on long duration missions in orbit should be one of health, not productivity.
The next question which needs addressing is “How much gravity does an orbiting habitat require?” Will a fractional G be sufficient to maintain an astronaut’s normal physiologic condition, or will a full one G be necessary? These questions are critical because they relate directly to the cost and complexity of a rotating habitat — the higher the gravity level required, the larger the habitat’s size and/or angular velocity.
What are the trade-offs when we use Artificial-G?
We must not forget that one of the major reasons we are going into space in the first place is to gain access to unique properties such as microgravity. Rotating habitats have many negative draw-backs which weigh against the medical benefits. Some of these include: numerous engineering complexities, danger of accident, loss of microgravity working environment, cost, environment, vibration, Coriolis forces, gravity gradients, docking complexities, and difficulties starting and stopping rotation.
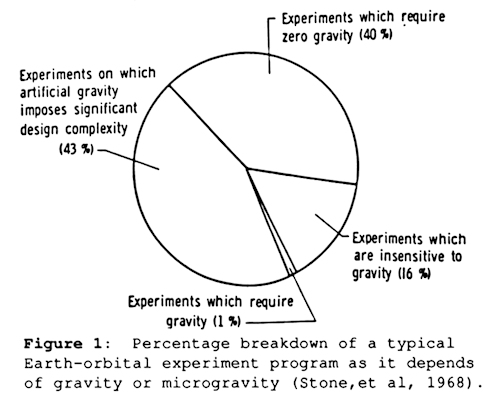
In the late 1960’s, an evaluation of the impact of artificial gravity on a typical Earth-orbital experiment program disclosed an interesting results (Figure 1) — while only 1% of the experiments required gravity, over 83% required zero gravity or would be significantly hampered by gravity (Stone, et al., 1968).
Any design for a rotating habitat must then include non-rotating facilities for microgravity work.
At this time it is worth mentioning that there are many significant benefits, in addition to the medical ones, which should be considered in the overall decision to pursue rotating habitats. In brief, these benefits include: improvement in ease of fluid and waste management, benefits to “orbital” agriculture, and potential benefits to crew psychological well being and social interactions.
Research in the area of Rotating habitats received serious consideration by NASA in the mid-late 1960’s when it was thought that a rotating manned facility would follow Skylab. It has been greater than fifteen years since the bulk of the work discussed in this paper was completed. At this time, when we are contemplating a return to the moon and a manned mission to Mars, it is necessary to reconsider and re-examine the issue of rotating habitats.
2. MEDICAL EFFECTS OF WEIGHTLESSNESS
On the macroscopic and microscopic level, humans have evolved to expect a constant acceleration of 9.82 m/sqsec on the body along different axes. Because of this, the human body has, in some ways, become dependent upon the gravity forces to maintain what is considered a normal state of health.
The physical condition of the body is continually changing to minimize stress, minimize energy use, and best suit the environment. The molding and shaping of muscles, bones, blood chemistry and even sensory reflexes is a dynamic process perhaps best described as “plastic”. It is common experience that exercise strengthens the muscles and cardiovascular system while bed rest or reduced physical activity causes the underused muscles to atrophy. It is not surprising then, that in microgravity, without the continual pull of one-g, the body adapts to the reduced stress by breaking down superfluous structure.
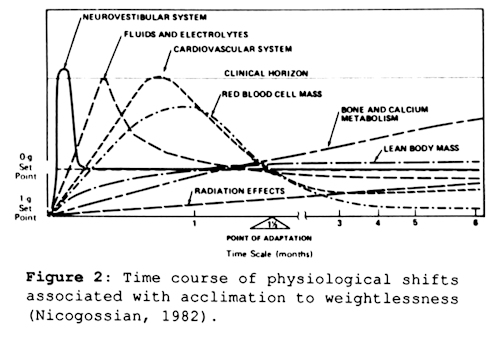
It is well documented that extended periods in space, including the planned crew rotation periods for the Space Station, lead to significant pathophysiologic changes in various systems of the body. Experience in the United States and Soviet space programs has demonstrated that exposures to microgravity, on the order of weeks, begin the processes of osteoporosis, cardiac deconditioning, general muscular atrophy and immune system suppression, while shorter stays produce body fluid shifts and vestibular adaptation (Nicogossian, 1982). On the whole, these problems cause little difficulty in space (except for space motion sickness and perhaps immunosuppression), but present a major problem for a crew’s well being and safety upon return to Earth’s one gravity or for work on Mars.
Experience with the long duration Soviet missions indicate that extended periods of up to eight months in orbit require over four weeks of rehabilitation on the ground before the crew returns to their baseline physiological status (Gazenko, et al, 1981). These extensive recovery periods stand as serious barriers to manned interplanetary missions and the potential industrialization of space. As concluded by the National Commission on Space, “We need a vigorous biomedical research program, geared to understanding the problems associated with long-term human spaceflight” (Pioneering the Space Frontier, 1986). Currently, three approaches are being used or considered as continuing countermeasures to the deleterious effects of microgravity: Physical exercise, lower body negative pressure, and drug therapy. Of these, exercise has been most successful.
Exercise on Skylab IV and the Space Shuttle involved use of the treadmill, bicycle ergometer and isometrics (Thornton, 1981). The daily exercise program, which lasts approximately two hours, addresses the cardiovascular needs but does not attend to osteoporosis, cephalic fluid shifts or the apparent immunosuppression. Further, it utilizes a significant portion of the crew’s potential work time, which is a highly valuable commodity. Because the physical deconditioning is caused by a lack of gravity, it would seem that the most effective way to recondition or prevent deconditioning of astronauts in space would be to provide them with artificial gravity such as that provided by large rotating space structures.
3. MEDICAL & SCIENTIFIC RATIONALE FOR ARTIFICIAL GRAVITY
The decision to build large rotating habitats of significant complexity and cost might be reasonable if it is shown that the pathologic effects of long-term space habitation can not be prevented or diminished through other less expensive means (exercise or drugs) . Economically, there will be a tradeoff between the development/construction costs of the habitat versus the rehabilitation costs associated with the recovery of crews following long-duration flights. Soviet scientists report that the three Salyut 7 cosmonauts who remained in space continuously for 237 days required approximately four weeks of recovery time on Earth to return to their preflight physical health. It is not known at this time whether stays in orbit of greater than eight months will result in any type of permanent damage either to the cardiovascular or musculoskeletal system, though this is not outside the realm of possibility.
Rationalizing the development of a Rotating Space Habitat is based significantly on the assumption that Artificial Gravity can stress and recondition the various systems of the body. Following is a summary of the pathologic effects to the major systems of the body:
Renal/Fluid shift
In microgravity, a significant cephalic shift of intravascular and extravascular fluids takes place. Experiments aboard Skylab have measured a shift of 1.5 to 2.0 liters occurring over a period of three to five days, reaching a peak flow rate after twenty-four hours (Hoffler, Bergman, & Nicogossian, 1977). More recent investigations on the Space Shuttle indicate that the cephalic fluid shift may occur more rapidly than previously thought, with the initial shift actually beginning on the launch pad while the astronauts are in a reclined (head-down) position. The maximal shift is evidenced by a calf girth decrease of nearly 30%, head congestion and associated facial puffiness (Thornton, Hoffler, & Rummel, 1977).
In adapting to this shift, the body’s homeostatic systems respond to the initial increase in central body volume by decreasing sympathetic nervous system tone and increasing urine output. These responses lead to a severe orthostatic hypotension seen upon return to Earth (Nicogossian, 1982) secondary to an extensive diuresis and an increased venous compliance.
Artificial gravity would be the simplest solution to the fluid shift and diuresis problem by preventing it from occuring in the first place, or reversing any initial shifts which might occur.
Cardiovascular
Cardiovascular deconditioning has been noted since the earliest space missions, manifesting itself as orthostatic intolerance (upon return to Earth) and changes in heart size. On Earth, blood passing through the lungs is confined largely to the lower two-thirds of the lung. In microgravity however, the blood redistributes itself throughout the lung.
This fluid redistribution, in addition to the fluid shift mentioned above, overloads the heart with blood and triggers an excretion of fluid and salts by the kidney. This diuresis of fluids (approx. 2 liters) in combination with a decrease in thirst leads to significant contraction of the intravascular space. After compensation has occurred, a decrease in heart chamber size associated with a 10 percent atrophy of heart muscle occurs.
This decrease in cardiac size causes an increase in heart rate (even at rest) which lasts throughout the mission. A decrease in the amount of exercise due to the absence of the resistive forces of gravity decreases the work load on the heart and may therefore lead to cardiac muscle atrophy.
Inflight Electrocardiogram monitoring of crew members engaged in extravehicular activities (EVA) indicates that the heart, following compensation, becomes more irritable and prone to arrhythmia (Sulzman, 1987). Artificial gravity has the potential to prevent these cardiovascular problems by preventing the decrease in intravascular fluid volume, and by increasing the average workload experienced by the astronauts as they function in a weighted environment.
Musculoskeletal
Both U.S. and Soviet manned missions have shown that bone and muscle atrophy in space crews is proportional to the length of time spent in microgravity. In general, muscle atrophy precedes skeletal atrophy with the greatest reduction in muscle mass occurring during the first month. Calcium loss begins slowly in the first week and increases gradually over the next several months with an average rate of O.5% per month (whole body loss rate) and a peak rate in some areas of bone of 3-5% per month (in weight bearing bones) (Donaldson et al., 1970). On the average, normal males have a bone density of 1.5 gm/sqcm (in the spine), and are at risk for bone fracture when the density approaches 1gm/sqcm.
A loss of this magnitude is conceivable for a person living in microgravity for a one to two year period. It is important to note that the overwhelming majority of the calcium loss is from the weight bearing bones. On the 84 day Skylab mission mineral losses from the os calcis was approximately -11.2% ± 5.5%, while no losses where noted in the radius or ulna (Smith, Rambaut, Vogel and Whittle, 1977).
Unlike other physiologic adaptations, the calcium loss (osteoporosis) occurring in the weight bearing bones during microgravity did not reach a plateau during the 84 day Skylab mission (see figure 2). Because of this, and consequences such as calcium/phosphate stone formation, and the forementioned fractures, it is crucial to tackle this problem. Currently it is not known what amount of stress (gravitational force) must be maintained on the weight bearing skeleton to prevent osteoclastic demineralization.
Experiments conducted on rats aboard the Cosmos-936 biosatellite support the thesis that artificial gravity provided by centrifugation can prevent osteoporosis. Centrifugation of the rats in orbit was found to prevent changes in calcium and phosphorus content of the long bones (Gazenko, Il’in et al., 1980) and also to prevent osteoporosis (Stupakov, 1981).
Work conducted by Jankovich and Lange who measured the effect of hypergravity (1.5, 2.0, and 2.5 g produced by continuous centrifugation) on the femur and tibia of rats over a period of two to ten months is of particular interest. Significantly, the investigators found no systematic changes in these rats. This finding is important because it suggests that there exists a threshold above which bone development is essentially normal and below which atrophy occurs (Jankovich, et al., 1971).
It may be that the threshold for humans is less than 1g (e.g. 0.5g), and therefore, a rotating habitat that provides one half Earth’s gravity is sufficient. It is more likely, however, that our musculoskeletal system has evolved to depend on 1g, and a lower g level will be inadequate. Determining the threshold is none-the-less worthy of investigation. Such work would be conducted on a Varible Gravity Facility such as proposed by the National Commission on Space.
Immune System Changes
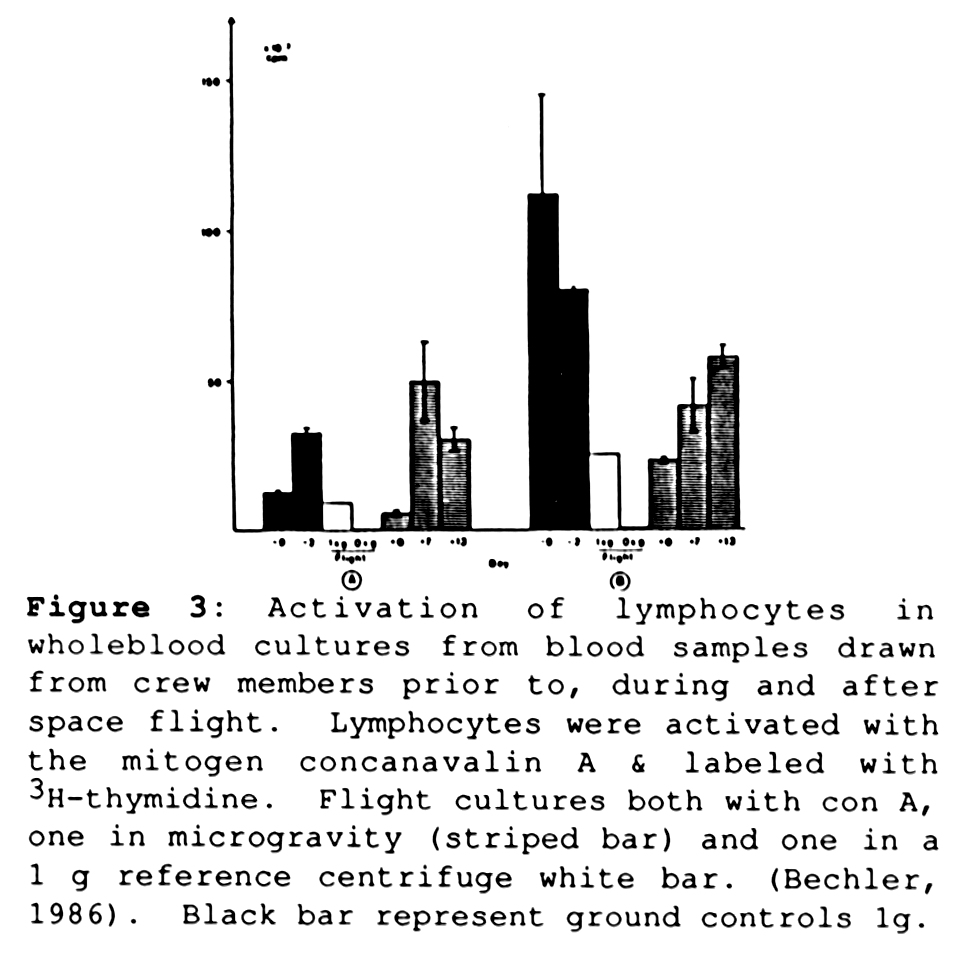
Microgravity is known to cause an atrophy of the bone marrow and the immune system leading to the so-called “space anemia” and a defect in the “T” lymphocytes. Experiments on Spacelab 1 found a surprising gravity dependence of the lymphocyte cells (a critical part of the human immune system responsible for the production of immunoglobulins and cell mediated immunity ) (Cogoli, 1984). Cultures of human lymphocytes exposed in microgravity to the mitogen Concanavalin A showed less than three percent of the activation of ground controls.
These results support the observation that lymphocytes extracted post flight from the majority of crew members on U.S. and Soviet space missions had a decreased response to mitogen after flight (returning to normal activity 7 to 13 days later) (Cogoli, 1986). Perhaps as important, experiments conducted on lymphocyte cultures aboard the D-1 mission discovered that these cells can maintain their normal functioning level in space by being provided with “artificial gravity” via centrifugation (figure 3) (Cogoli, 1986).
The significance of this possible “space-immunosuppression” goes beyond the danger of a simple infection. In particular, T cells also help fight off growing neoplasms, and a suppression of this system may hamper the astronaut’s ability to fight off a cancer while in orbit — a serious hazard in the high radiation environment of space.
Reproductive Capability
For those interested in colonizing space, a critical questions which has yet to be answered is whether human embryo development (gestation) can occur in fractional or microgravity. To date, no conclusive experiments have been conducted to address this issue. The Soviets have attempted to conduct mating experiments using mice, but were unsuccessful for unknown reasons.
Some indirect experiments, however, do bear significantly on this issue. In particular, experiments such as Cogoli’s work on lymphocytes, which indicate the sensativity of cellular and subcellular processes to gravity, begin to raise serious questions on whether the complex process of embryo-genesis can occur without any deviation in a microgravity environment. The answer to this important issue remains to be found by orbital experiments using animal models.
4. THE PHYSICS OF ROTATING HABITATS
There are four major features of a rotating habitat that cause artificial gravity to be different from real gravity. They are:
- Artificial Gravity Level (feasibility of hypogravity)
- Gravity Gradient
- Coriolis Forces
- Cross-coupled angular accelerations
Artificial Gravity Level: Radius and Angular Velocity
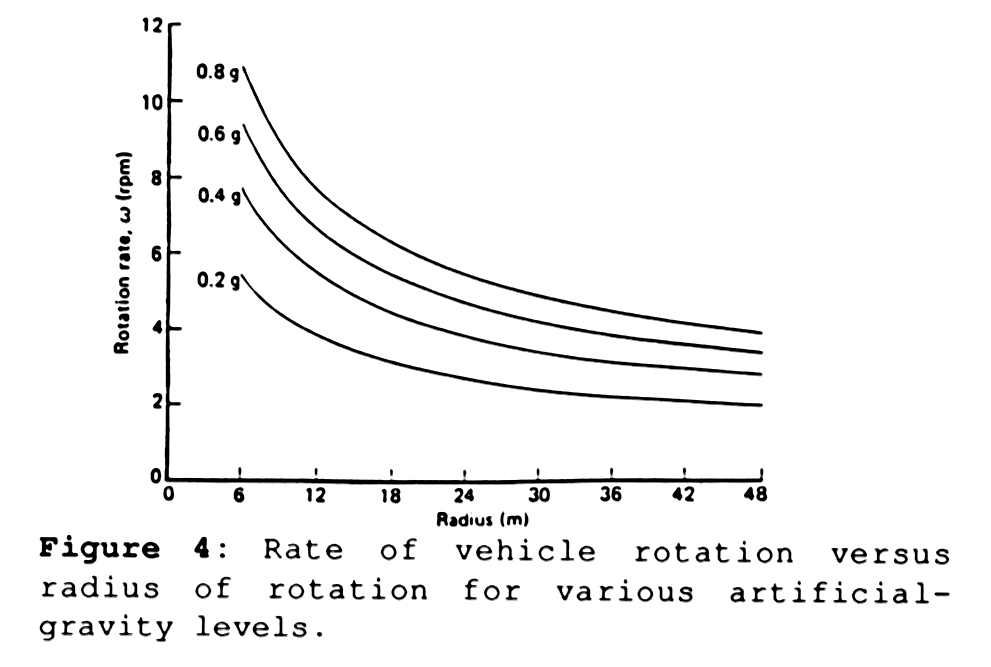
The centripetal acceleration (a) (m/sqsec) produced by rotation, refered to in this paper as “artificial gravity” is dependent upon two parameters of the rotating structure: Angular velocity (w)(rad/sec) and radius (r)(m) . In particular:
a=w2r.
This equation, graphed in figure 4, provides a fixed relationship between rotational speed and radius. As will be discussed later, a specific increase in artificial gravity level can be achieved either by increasing the radius, or by increasing angular velocity. This translates to a trade off between cost and complexity (which depends on the radius) vs. physiological/ psychological concerns (which depend on angular velocity).
G-gradients
Because the centripetal acceleration is a linear function of radius, there is a linear 100% gravity gradient which runs from the center of the habitat to the outer rim. From a physical standpoint, an object would weigh more on the floor than on a shelf. An object weighing 10 kg on the floor of the rotating habitat would be weightless in the center, and would weight 5 kg at a distance midway between the center hub and the outer rim (the floor).
The percentage weight change that an object undergoes during translation from Ra to Rb is described by DW/W = (Ra-Rb)/Rb. Thus an object lowered a total of one meter in a 20 meter rotating station (from Ra=19m to Rb=20m) would have a 5% change in weight.
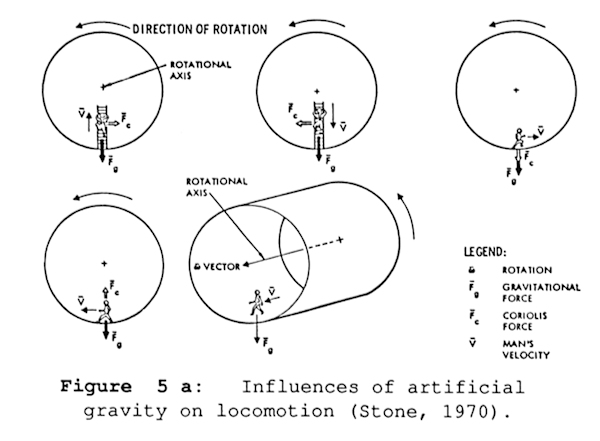
Influence of Coriolis forces, on limb motion and locomotion
By far the most bizarre affects are caused by the Coriolis force. A Coriolis force is an apparent force that is applied to an object moving linearly within a rotating system. The Coriolis force has a magnitude of 2•wxV ( w cross product with V) where w is the angular velocity of the rotating environment and V is the linear velocity of the moving object. Any object moving in a direction not parallel to the axis of rotation will experience Coriolis forces.
Consider the individual ascending the ladder in the first frame of figure 5a. Evaluated in terms of angular momentum, the astronaut’s reduction in rotational radius is accompanied by an increase in angular velocity (Thompson, 1965). As the astronaut moves into an area of “reduced velocity” he/she decelerates, in effect, is forced toward the leading edge.
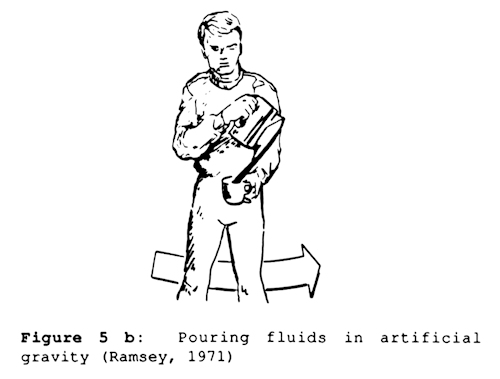
As demonstrated in figure 5a, a person moving radially downwards will be forced towards the trailing edge, a person running in the direction of rotation will get heavier, and a person moving counter to the rotation will become lighter. No moving object is immune to Coriolis forces, even a moving fluid deviates from its expected path due to Coriolis accelerations (figure 5b
Vestibular Coriolis Cross-coupling
Movements of the subject which result in functional disturbances fall mainly into two categories: rotation of the head out of the plane of rotation of the room and whole body movements. The former generate very small inertial forces and their effect, at least when the subject is near the center of the rotating environment, would be negligible were it not for the semicircular canals.
The canals are so structured that the sensory elements are stimulated by the gyroscopic forces, and the bizarre pattern of the stimulus is the essential factor causing the symptomatology of canal sickness. The Coriolis cross-coupled angular accelerations (which cause the gyroscopic forces) occur within a rotating environment when an angular motion is made about an axis not parallel to the system axis of rotation (w1 x w2). These accelerations produce a torque to the moving object about an axis perpendicular to the axes of rotation of the environment and the object.
The semicircular canals are three mutually orthogonal fluid-filled toruses which are able to detect pitch, roll, and yaw movements of the head. The turning or nodding of the head in a rotating environment generates cross-coupled angular accelerations that induce motion of the fluid within the semicircular canals not normally stimulated by such head movements in a stationary environment. This results in illusionary sensations of bodily or environmental motion. The intensity and duration of the symptoms appear to be related to the individual’s tolerance threshold to the vestibular stimuli. (Green, 1971).
5. LIMITATIONS FOR ROTATING HABITATS
What minimum radius provides acceptable G gradient?
The gravity gradient appears to be the problem of “least concern” in designing a rotating habitat. When examining the gravity gradient problem and its effect on the inhabitants of a rotating station, a benchmark useful for comparisons, is the percentage weight change which occurs when an object is moved from a person’s eye level to their feet (a drop of ~1.5 meters) in other words, how much heavier does an object get when it is lowered from head to foot level.
If one considers 20% an uppermost value, then the minimum radius allowed for the habitat would be 7. 5 meters (which would require an angular velocity of approximately 8 rpm to achieve 1 gravity acceleration). Gravity gradients of any significance (e.g. greater than 20%) will be intrinsically avoided because they require habitat designs using small radii and large angular velocities to produce significant g levels.
Motion sickness due to Coriolis Cross-coupled Accelerations
Movement of a subject within a rotating environment gives rise to bizarre stimulations of the vestibular, visual, and proprioceptor systems. The interaction of the environmental stimuli on these sensory systems may produce symptoms of vertigo, disorientation, lassitude, postural aberrations, or perhaps, ultimately, nausea, described as motion sickness, space sickness, or canal sickness.
It has been demonstrated that many test personnel subjected to rotation in the Pensacola Slow Rotation Room respond with a deteriorization in well-being, frequently associated with a feeling of increasing lethargy (Green, 1971). As will be discussed later, adaptation (and subsequent immunity) to this “Coriolis sickness” has been shown to occur for rotation speeds less than or equal to ten rpm. No Coriolis sickness is noted for speed of one rpm or less.
Walking in an Artificial Gravity Environment
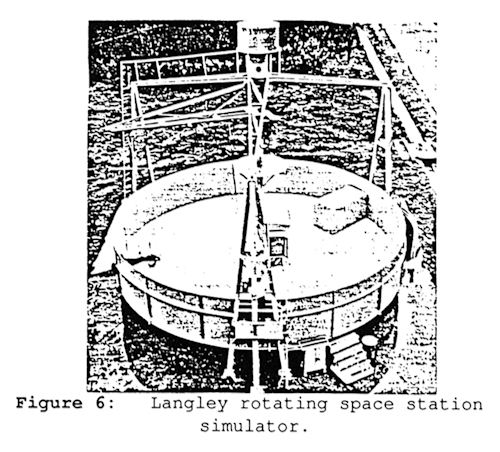
Research addressing the effects of rotation on man’s walking abilities on circular and flat walls was conducted in 1971 at the NASA Langley Rotating Space Station Simulator, a circular platform of 12 m diameter with a 1.8 m vertical wall at the periphery. During rotation of the simulator, subjects were suspended horizontally by a servomechanized boom and allowed to “walk on the walls”. Rotation speeds varied from 3 to 10.5 rpm, corresponding to g-levels from 0.05 to 0.75 g at the subject’s feet.
It was found that walking in the direction of rotation at a level between 0.167 – 0.3 g was most comfortable. At levels above 0.3 g, the subjects reported sensations of leg and body heaviness which are reported to quite disturbing at levels above O.5 g. At the lowest level tested, 0.05 g, it was found that walking opposite to the direction of rotation was not possible, while walking in the direction of rotation was possible (Letko, 1971).
6. THE QUESTION OF ADAPTATION
For a rotating station of reasonable size (e.g. radius of 20-30 meters), the gravity gradient is not a critical issue, rather, motion sickness due to cross-coupled Coriolis stimulation and the deviation of limbs during movement pose the major problems which must be resolved.
Pensacola Slow Rotating Room Experiments
Over the past 30 years, scientists and physician have carried out a great number of experiments to investigate the effects of continual rotation at varying angular velocities on human physiology and performance. These experiments have exposed subjects to rotation rates as high as 20 rpm, and at lower velocities for periods as long as 25 days. The majority of these experiments have used the Pensacola Slow Rotation Room (SRR), a multisided windowless room 5 meters (15 feet) in diameter and 2.5 meters (7 feet) high with a square center post.
The stressful and disorienting stimuli encountered in a rotating environment occur only when subjects moves their head outside the plane of rotation. Limiting head motion would significantly reduce the unpleasant stimuli, but this would severely hamper normal activities, and slow or prevent adaptation to the rotating environment from occurring. Two important factors govern the appearance of symptoms in subjects: first, the susceptibility of the unprotected subject, and second, the angular velocity of the room.
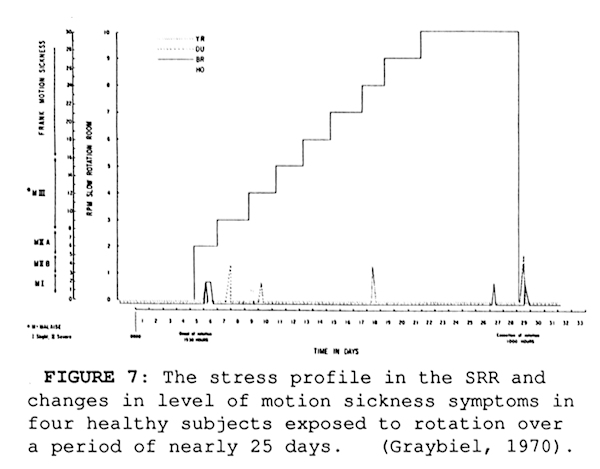
With regards to the latter, even subjects highly susceptible to vestibular side effects are not handicapped on sudden exposure to 1 rpm (Graybiel, 1975). Graybiel and his coworkers found that some individuals could adapt and function in environments rotating at rates as high 10 rpm, but that the ability to adapt varied drastically from person to person, taking as long as two weeks to occur, and causing a great deal of unpleasent motion sickness during the process for some. A number of experiments conducted in the Pensacola Slow Rotation Room addressed the problem of how to more rapidly and more comfortably bring about adaptation.
One set of experiments attempted to prevent motion sickness by incremental steps in the angular velocity to a terminal velocity of 10 rpm. Numerous increments over various time schedules were tried unsuccessfully. Of those attempted, the only adaptation schedule which was able to provide a symptom-free adaptation to a 10 rpm rotational velocity was a nine step increase over a period of 25 days (Graybiel, 1971).
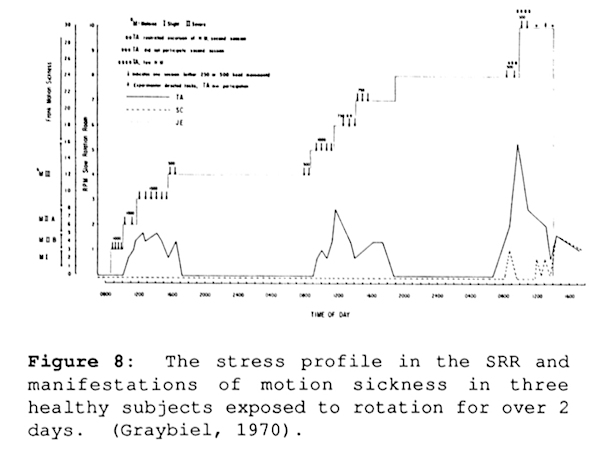
A second series of experiments combined the stepwise approach to the terminal velocity with the execution of active head and body movements.
At each 1 rpm step, the subjects were required to make 1000 head movements taking slightly more than half an hour. In a two-day experiment which examined the efficacy of an adaptation schedule, three subjects were rotated up to a speed of 10 rpm in 1 rpm steps.
At each step approximately 1000 head movements were executed. Two of the three subjects suffered few side effects, while the third was quite susceptible, becoming very drowsy at 2 rpm, experiencing epigastric discomfort at 5 rpm, and minimizing or refraining from making head motions at the higher rpm (Graybiel, 1971).
These findings suggest (in the case of 2 out of the 3 subjects) that the time required to effect adaptation can be greatly shortened by setting up an adaptation schedule for controlled head movements and stepwise increases in angular velocity. They also suggest that were it possible to precisely control the angular velocity of a rotating habitat, adaptation to high rpm could be accomplished in a less stressful manner.
For completeness, it is worth mentioning an experiment conducted in the SRR which sought to determine if individuals were more susceptibile to vestibular side effects when adapted to rotation while standing parallel to the axis of rotation versus when adapted while standing perpendicular to the axis.
In these experiments, conducted at 4 rpm, one group of subjects underwent adaptation in the horizontal mode — “walking on the walls” of the SRR - and a second group underwent adaptation in the vertical mode. The findings indicate no significant difference in susceptibility between the two modes. In addition, subjects who adapted in one mode transfered their adaptation to the other mode without difficulty.
Motion Sickness and the “Conflict Theory”
The motion sickness developed by subjects in the Slow Rotation Room is very similar in nature to Space Adaptation Syndrome, the motion sickness developed by astronauts in the microgravity environment. If it is the case that adapting to either environment yields immunity to the other, then this would bode well for rotating habitats allowing individuals symptom-free transitions from microgravity to the rotating habitat and vice versa.
The “conflict theory” is the currently accepted explanation for the cause of motion sickness. In general, the theory states that an environment which presents conflicting sensory signal to the Central Nervous System (CNS) will cause the symptoms of motion sickness (Reason, 1978; Oman, et al., 1986).
A person below deck on a boat, for example, suffers seasickness because the vestibular system picks up the swaying of the boat, but their eyes which are fixed to the head, and consequentially to the boat, perceive a stationary environment. “Sensory conflict” signals result when the actual sensory signals are compared to expected ones based on previous experience or an internal model (Reason, 1978).
The otoliths, which are the structures in the vestibular system which normally detect the gravity vector, are thought to be responsible for Space Motion Sickness (Space Adaptation Syndrome). The conflict in Space sickness is between the otoliths which, in space, interpret the lack of gravity as “free fall” and the eyes which observe a stationary environment. As a final example, Coriolis sickness derives its “sensory conflict” from the semicircular canal, the otolithic and the visual cues. In this case, the eyes and otoliths detect a mere tilting of the head, while the semicircular canal detect a bizarre pattern of stimulus as one canal exits the plane of rotation and another canal enters it.
An objective result of Space Adaptation Syndrome and Coriolis sickness is that it disappears after a period of two to four days — the subject “adapts” to the environment. The critical question here is why? Adaptation could either be the result of sensory/motor learning (in which the internal model of expected relationships between the various sensory inputs is updated), or it could be due to a modification of the sensitivity and threshold of the emetic and autonomic centers of the brain — a fatiguing of the output systems in motion sickness (Oman, 1982).
If this second explanation is correct and the threshold of the emetic centers are modified, then this translates to a “generalized immunity” to conflict signals. Such a “generalized immunity” has been noted in Earth-bound experiments. For example, subjects “over trained” for Coriolis sickness in a rotating chair show a decreased susceptibility to other types of provocative stimuli (though not a total immunity).
Generalized immunity, if it exists would solve many of the problems seen with rotating habitats. In particular, an individual who enters microgravity and proceeds through the three or four day period of Space Adaptation Syndrome might then have acquired an immunity which would allow motion sickness-free adaptation to a rotating habitat and symptomless travel between the two environments. This particular thesis is one explanation for the results of M131, an experiment conducted on Skylab 2, 3, and 4 to investigate the susceptibility of astronauts in the weightless environment to motion sickness induced by cross-coupled Coriolis stimulation.
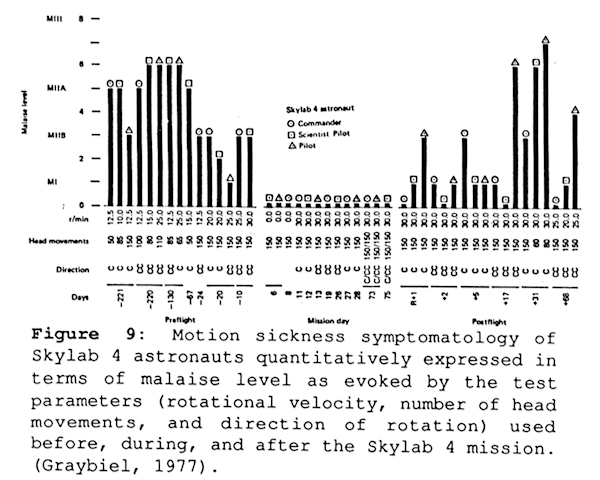
Subjects in the M131 experiment received vestibular stimulation by conducting 150 rhythmic head movements in a rotating chair traveling at angular velocities between 12 and 30 rpm. Skylab astronauts were tested for susceptibility preflight, during the mission, but not until after mission day 5, and postflight (as soon as Return +1).
In general, for all astronauts tested while in orbit, the M131 experiment demonstrated an immunity to motion sickness as caused by head movements in a rotating environment. The astronauts who had been susceptible while on the ground were virtually symptom free in space, even when the angular velocities were increased to 30 rpm. In addition, the crew of Skylab 3 and 4 demonstrated a postflight immunity to rotating-chair-induced motion sickness which lasted for two days and five days respectively (Graybiel, 1977).
What is critical in this experiment is that it did not begin until day 5, after vestibular (or neurological) adapation to the microgravity environment had already occurred. The alternative explanation to the generalized immunity thesis is that the signals from the otoliths (a cause of the conflict signal) were no longer present at the start of the experiment on day 5 because of the lack of gravity. This however does not explain the post-flight immunity seen by the astronauts of Skylab 3 and 4.
Transitions between zero-G and one-G
If the concept of a generalized immunity affording common protection for space motion sickness and Coriolis sickness is incorrect, it might still be feasible to have individuals make repeated transitions between the two environments without having to adapt to the new environment each time. In particular, the question which must be addressed concerns an individual’s ability to maintain two “mind-sets” — one for the rotating environment and one of zero gravity.
Evidence which points towards the need for repeated adaptation has been seen in two circumstances. In experiments using the SRR, it had long been observed that normal persons with mild symptoms resulting from exposure to Coriolis accelerations, experience an aggravation of motion sickness on cessation of rotation. In a somewhat related circumstance, astronauts returning to Earth after adapting to the weightless environment of space have experienced dizziness and motion sickness.
The stronger evidence however is found for the argument that astronauts will develop two “mind-sets” one for the rotating environment and one for the zero gravity environment. Some insight into this question comes from the understanding that there is precedent for the central nervous system’s ability to maintain multiple mind-sets. Common examples of this include vision with and without eyeglasses for those individuals who wear them. Functioning on foot, behind the wheel of a car, or behind the controls of a plane. In each of these situations, the visual, vestibular and prioceptive inputs are unique yet transitions from one to another occur without difficulty.
Adapting to Limb Movement Deviations
If the design of a rotating habitat requires a high angular velocity (e.g. above 4 rpm), then coriolis forces on ordinary hand movements will be noticable and perhaps disturbing. The human central nervous system (CNS) has as one of its greatest assets adaptability, sometimes referred to as “plasticity”. Because of this, it has been able to survive and excel in novel circumstances which it has never before encountered.
The Coriolis forces present on a rotating habitat will provide a significant challenge to the CNS, specificially the hand-eye coordination system. The question here is whether the CNS can adapt to limb movements in this new unusual force field where each movement forward is accompanied by a force due to the Coriolis force.
In one sense, hand-eye coordination undergoes adaptation during each transition between one G and microgravity. On Earth, the central nervous system’s “control equation” for the hand must take into account the arm’s weight. In microgravity however, the “control equation” must be changed to take into account the lack of weight — this is reported to occur very rapidly. I will refer to this type of binary adaptation (weighted arm vs non-weighted arm) as primary adaptation. In a rotating environment, a moving arm must contend with the Coriolis acceleration in addition to the gravitational and centripetal acceleration.
The Coriolis acceleration is of particular interest because, unlike gravitational or centripetal acceleration, it is dependent both on the velocity of the hand and the plane of movement of the hand relative to the axis of rotation. Dr. Ashton Graybiel, in his Slow Rotation Room experiments, found that individuals who remained standing in one particular orientation in a rotating room could, after a period of learning and adaptation, throw darts consistently. These individuals, when adapted, could move their arm at any velocity without significant deviation — in essence, they had added to the “control equation” for their arm a term which was velocity dependent. This type of adaptation to a dynamic factor (in this case velocity) will be referred to as secondary adaptation.
It should be pointed out that when arm velocities are not large, and arm translation distances small, Coriolis deviations of the limb movement will not be significant. This was clearly pointed out by O’Laughlin and coworkers who found that individuals spinning in a centrifuge at 12.2 rpm (head and body fixed) were precisely and accurately able to push buttons over a hand translation distance of 20 inches and no measurable effect due to the Coriolis force was found (O’Laughlin, T.W. et al., 1968).
A third level of complexity for control of a moving limb in a rotating environment exists if we remove the constraint that the subject stand in one particular orientation. In reconsidering the dart throws, if the subject is allowed to move so that he/she throws the dart at different angles to the axis of rotation (of the environment), then the cross product of the arm’s velocity and the angular velocity vector would vary. Consequently, the forces on the arm would be different for each new direction and adaptation would become more difficult.
The type of adaptation to both a dynamic factor (velocity) and an orientation factor I refer to as tertiary adaptation. In order for a person to undergo tertiary adaptation they would have to add into the “control equation” for the arm, a velocity dependent term and a term which accounts for the plane of movement of the arm relative to the plane of motion of the rotating environment.
Needless to say, this is a substantial demand to make on the central nervous system. What is perhaps most difficult about undergoing tertiary adaptation is that, at any particular time, one would not necessarily be aware of which direction the axis of rotation is pointing. This is analogous to a person in an enclosed room on Earth, being unaware of which way is north, east, west or south. One suggestion made to solve this, is that all the walls on the rotating habitat be painted colors which relate to the axis of rotation.
7. A REVIEW OF PREVIOUS WORK: THE ROCKWELL ROTATIONAL TEST FACILITY
One particular study on the effects of long duration rotation is outstanding for the depth of investigation. The study conducted by North American Rockwell Space Division examined the effects of seven days of rotation in a centrifuge designed to simulate a space station.
In April of 1969 NASA released a Request For Proposals (RFP) to develop a rotating “Space Base” (NASA RFP 10-7192).
“Space Base will provide artificial g and zero g environments in separate volumes simultaneously. For example, the principal living quarters, command and control stations, and some laboratory space may be located in the rotating arm for the effectiveness, comfort, and convenience of the crew.”
“Acceleration levels in the main operating and habitability volumes will be between 0.3 and 0.7 times gravity. The nominal rotational rate will be 4 rpm.”
In response to this RFP, North American Rockwell developed a rotational test facility capable of conducting artificial gravity tests at 3, 4 and 5 rpm with a crew module located at a mean radius of 22 meters (75 feet). The crew module with internal dimensions of 3 m by 12 m (10ft by 40ft) automatically swung out during rotation to provide a walking surface normal to the total gravity vector. The module was equiped with four bunks, a toilet, shower, lavatory, kitchen-recreation area, and a psychomotor test area.
In addition to the crew module, the facility was equipped with a movable enclosure (“walking room”) that could be positioned at radii of 20 (6m), 40 (12m), 60 (18m), or 70 feet (21m). In this room, the test subject was supported by a sling system which countered the pull of the Earth’s gravity field, and allowed the subject to freely walk on the walls (a surface 2.5 meters in length). The subject was permitted to walk tangentially in either the “pro-spin” or “anti-spin” directions. Weighted boxes present in the room were manipulated to examine the ability to handle objects.
The Rotational Test Facility (RTF) was instrumented with equipment capable of monitoring the physiological and psychological effects of long-duration rotation. In particular, subjects were monitored for electrocardiogram, electroencephalogram, and blood pressure changes. In addition, a complete battery of psychomotor tests to evaluate fine motor control, dexterity, short term memory changes, and changes in vision was performed.
Four subjects were selected for the RTF program after undergoing an extensive physical and psychologic evaluation, including susceptibility to motion sickness. It is important to note that subjects immune to motion sickness were preferentially selected. After a series of twelve one-day tests, performed to examine the facility’s readiness, the four subjects underwent rotation at 4 rpm for seven days, in a full scale experiment.
Biomedical and Psychomotor Results
The biomedical results were unremarkable; no significant trends in either heart rate or blood pressure were noted during the seven-day test. Further, there was no increase in orthostatic tolerance or work capacity, as had been expected in response to the greater loading of the increased g forces. The psychomotor tests, on the other hand, showed a number of important results. First, performance improved over test days, but adaptation could not be reliably distinguished from learning.
It was seen that adaptation or recovery to pre-test performances occured within two days, and learning and/or adaptation occured throughout the seven day period. Second, there was a considerable difference between test subjects. Two of the four subjects proved to be very immune to effects of rotation, and performed nearly perfectly during the seven days. The other two subjects had their psychomotor scores significantly reduced during the first two days of the seven day test. Third, performance was fastest at the hub, and slowed down as a function of increasing radius (increasing G level).
Locomotion
The results from the study of locomotion in the “walking room” paralleled many of the results found by Letko on the NASA Langley Rotating Space Station Simulator (Letko, 1971). In particular, it was observed that walking in the pro-spin direction was consistently easier. Subjects described increased body control and an easier ability to start and stop, even at g levels as low as 0.1g. At a g level of 0.2g’s (40 feet and 4 rpm), it was found that walking in either direction was acceptable.
It is worth noting that performance and confidence continued to improve over the seven-day test period. Walking at a O.6 g-level (70-foot radius at 5 rpm) was described by subjects as a very “Earth-like” situation with respect to balance and work. The most comfortable conditions, from the subjective viewpoint, were at a 60-foot radius at 4 rpm, which produced an 0.3 gravitational force. All activities at the 20-foot station, even at 5 rpm (0 .17 g’s), were both uncomfortable and unstable.
Radial Transfers
An elevator and a ladder were used for radial locomotion between the crew module and the hub. Subjects found radial locomotion did not produce any excessively stressful stimuli in the vestibular system. In addition, they found that traversing the beam from one end to the other and passing through the axis of rotation caused no problems or discomfort. The use of the elevator was reported to be subjectively ideal, though a ladder was managable.
Recovery & Ataxia
Within two to four hours following “despin”, the subjects began to consistently perform up to the pre-rotation baselines on the psychomotor tests. Readaptation continued for at least an additional 24 hours before all symptoms of ataxia disappeared. It is worth noting that the test subjects were all surprised at the lack of severe symptoms after rotation ceased.
Conclusions
At 4 rpm and a radius of 22 meters, subjects in the crew module experience the vector summation of 0.4g (centripetal acceleration) and 1g (Earth’s gravity) for a total of 1.08 g’s. In orbit, a similar facility would have provided subjects with O.4 g. Whether this level of acceleration is sufficient to prevent physiologic deconditioninq remains to be seen. This study can only draw conclusions on the habitability of a facility with these parameters.
Based upon the results, it was concluded that, “the ability of the test crews to function with a high degree of proficiency and demonstrate good morale and cooperation, without motion sickness, was a pleasant surprise. Problems associated with eating, sleeping, etc., which had been predicted for the rotational environment, did not occur.” It must be remembered that the subjects who undertook this experiment were specifically chosen for the immunity to motion sickness.
These results may not apply to the general population.
8. NEW EXPERIMENTS AND PROPOSALS
Large Variable Radius Centrifuge (LVRC)
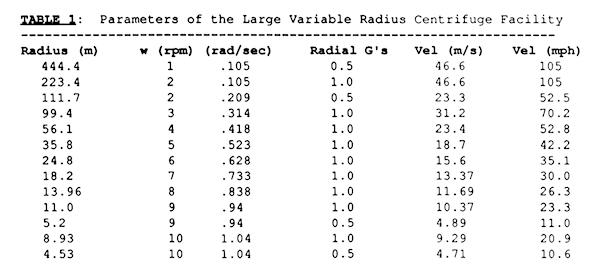
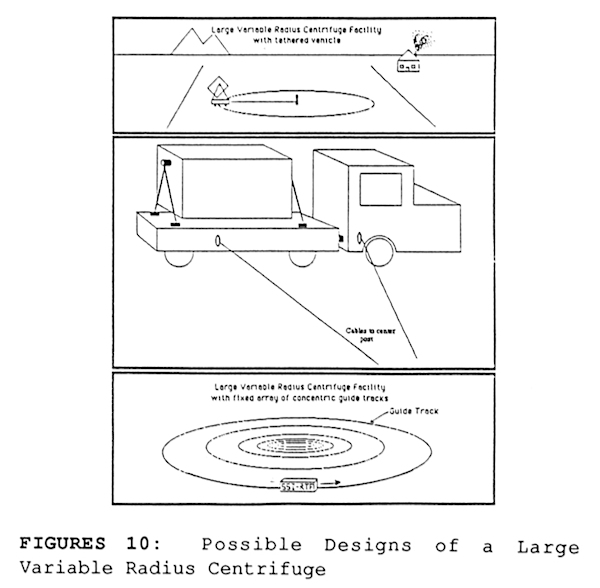
The experiments conducted using the North American Rockwell Rotational Test Facility began, but did not complete, a very important direction of research which would allow us to gain the experience needed to build the first rotating habitats. At this time, I would like to propose the construction of a “Large Variable Radius Centrifuge (LVRC)” facility which would have a variable radius between 5 and 450 meters and a range of angular velocities between 1 and 10 rpm.
Experiments conducted on the LVRC would be a prelude to the work conducted on orbit by the Variable Gravity Research Facility proposed by the National Commission on Space. In particular, the LVRC would continue and expand on the work conducted by North American Rockwell’s Rotational Test Facility. Experiments performed using the LVRC would examine rotational velocities as low as 1 RPM and as high as 10 RPM (Table 1). They would also expand the population of subjects tested on the facility to reflect that of the user community (academics, construction workers, … ) rather than an elite “test pilot” community selected for their immunity to motion sickness. Experiments would also be designed to distinguish between learning and adaptation when testing psychomotor performance as a function of time on the rotating habitat.
The LVRC could be realized with a pivoting room mounted on a flat-bed truck. The truck would be tethered to a center post via a cable of variable length (Figure 10). Alternatively, the Large Variable Radius Centrifuge could be constructed using a series of concentric tracks. A crew module could be mounted onto any given track to conduct experiments at various radii. The tracks used in this configuration could be as simple as a monorail system or employ advanced technologies such a magnetic levitation.
Artificial Gravity Sleeper
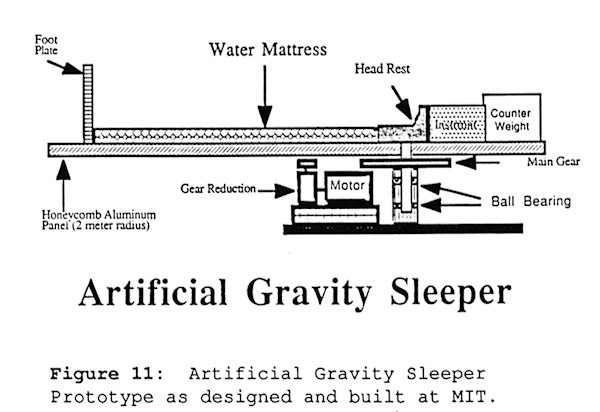
On the opposite end of the spectrum from the large radius, slowly rotating, space habitat is a device I am investigating at MIT’s Man-Vehicle Laboratory called the Artificial Gravity Sleeper (AGS). The AGS system is a 2 meter radius centrifuge designed to rotate a subject about an axis through the head, providing a centripetal acceleration gradient (100% gradient) which is maximal in the feet and zero at the head. The AGS is being evaluated for its ability to provide physiologic conditioning to an astronaut during sleep, as well as for its ability to enhance exercise by providing a gravity gradient for an astronaut to work against. For a 1.66 meter tall person, the AGS is rotated at a speed of 23.2 rpm to provide a one gravity acceleration at the foot plate.
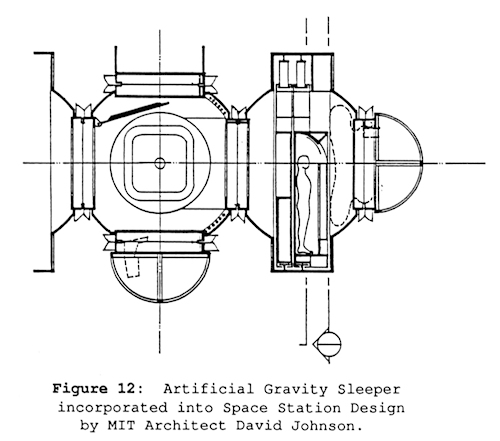
The AGS system is designed for use on Space Station (figure 12) but would be equally of value on the Lunar or Martian surface. It is hypothesized that rotation during sleep will help reverse fluid shifts, maintain vascular tone, provide centripetal acceleration for T lymphocytes, and afford some stress to the skeletal system. The AGS would also be equipped with a “cycle ergometer” and a device for “simulating stair climbing” in order to further condition the muscular, cardiovascular, and skeletal systems.
The difficulties associated with cross coupled Coriolis accelerations on the AGS are reduced by using a heated water mattress to reduce body movements during sleep, and a comfortable headrest to limit the head’s ability to rotate in yaw (Figure 11).
Fraction-G facility with one-G jogging track
One interesting prospect for keeping the radius and angular velocity small while getting the added benefits of a high artificial gravity level is that of using a half-g rotating habitat with a “one-g jogging track”. On such a facility the people would live, work, and sleep in one-half gravity, but for a few short periods during the day (total time of approximately half to one hour) they would jog around a track in the direction of the habitat’s rotation.
This would have the effect of increasing their angular velocity and thereby providing additional g-stress. The type of facility capable of this prospect would need to be a torus, with a continuous strip of track. For example, a 20 meter radius torus rotating at 4.73 rpm would develop 0.5 g at its outer radius. If an individual were to jog in the direction of rotation at approximately 9.3 miles per hour (4.1 m/s) their body would perceive a one gravity acceleration radially (through their feet).
This facility would be particularly appealing if it is found that a fractional g-level is sufficient for most human needs while a high g-level is needed to sustain normal physiologic tone in only one particular system. For example, it might be the case that O.3 g is sufficient to prevent a fluid shift (and subsequent diuresis) while 0.8 g is needed to prevent bone decalcification. In such an instance, it would be possible to provide both levels in the fashion described above.
Planetary Surface Rotating Habitats
There is no guarantee that lunar gravity will prevent any of the physiologic deconditioning which occurs in microgravity. In fact, it may be the case that the same difficulties seen with the cardiovascular, musculoskeletal, and immune systems in microgravity are also seen on the surface of the moon. This is of particular concern for those inhabiting the “lunar colonies” of the future in which people plan to spend the majority of their lives and raise families.
After a critical period of time, individuals on one sixth gravity lunar colonies might not be able to return to the stressful one gravity of Earth. One possible solution for this scenario is the rotating habitat. Such a facility would provide one g centripetal acceleration as a supplement to lunar gravity. It is significant to note that a similar facility might be needed on the surface of Mars if 1/3 g is not found sufficient to maintain physiologic tone.
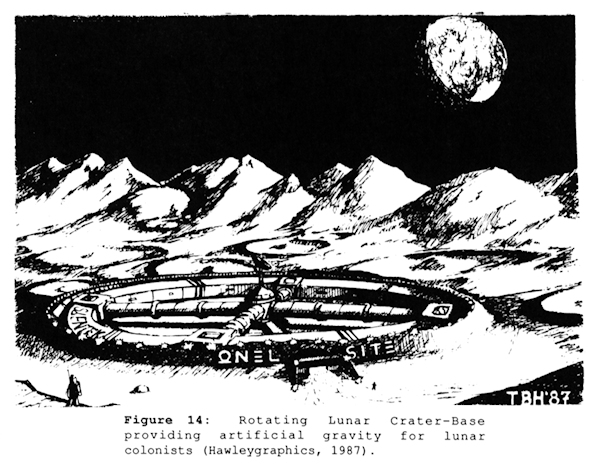
Figure 14 shows a rotating Lunar “Crater-Base” designed by Todd Hawley. This particular base uses a natural lunar feature - a 150 meter radius crater — as the guide for a magnetically driven torus rotating at 2.42 rpm.
9. CONCLUSIONS
A review of the pathologic effects of long duration stays in space reveals a significant amount of deconditioning which, to date, has not been prevented by exercise or drug therapy. This deconditioning could potentially stand as a significant barrier to interplanetary missions, space industrialization, and the eventual colonization of space. Rotating habitats providing artificial gravity to individuals living in space, have the potential to maintain the physical health and tone normal to people on Earth. At this time there is sufficient reason to warrant extended research on the topic of artificial gravity specifically towards answering these questions:
- What is the maximum angular velocity which an average group of individuals can adapt to? Over what period of time? With what degree of discomfort?
- What is the minimum gravity level required to maintain the normal physiologic functioning of each of the body’s major systems? What percentage of a person’s day must be spent at this g level to ensure normal functioning?
- Can mammals reproduce in microgravity? What level of G is sufficient? If not, can they reproduce using artificial gravity (centripetal acceleration)? How does Coriolis forces and gravity gradients effect the developing embryo?
The investigation of these issues will require the development of two new facilities. The first is a “Large Variable Radius Centrifuge” facility which can provide Earth-bound subjects with 1g centripetal acceleration at speeds as low as 1 – 2 rpm, and the second, is the orbiting Variable-G Research Facility recommended by the National Commission on Space in their final report. If the human species is to settle the space frontier in a permanent fashion, it is imperative that we understand exactly what are the gravity requirements and tolerances of the human body.
To date, the research conducted on Earth aimed towards establishing the maximum angular velocities sustainable by humans has provided three points of reference. First, that a speed of one rpm is not disturbing even to those subjects who are highly susceptible to vestibular effects; Second, at a speed of four rpm, some individuals will be naturally immune to motion sickness and others will have motion sickness but will adapt after a few days time and suffer little decline in performance; third, speeds of ten rpm will cause Coriolis sickness in most individuals if the transition from a stationary environment to the ten rpm environment is abrupt. Subjects can adapt to ten rpm if a schedule of stepwise increases in angular velocity and planned head movements is followed.
At this time it remains unclear whether individuals will have difficulties with frequent transitions between microgravity and the rotating habitat. While there is evidence to support the thesis that people in microgravity undergo generalized adaptation which protects them from both space motion sickness and Coriolis sickness, this is not proven and required additional investigation. Alternatively, it might be possible that space inhabitants adapt separately to both the microgravity and rotating environments developing two mindsets.
The most complete simulation of a rotating habitat was conducted by North American Rockwell Space Division which rotated four men for seven days at a radius of 22 meters. The study concluded that there were no biomedical abnormalities, spirits were high, and only two of the four subject had problems for the first two days. It is unfortunate, however, that the study was limited to an elite group of test subjects chosen for their immunity to motion sickness.
Finally, it is worth noting that rotating habitats may be necessary on a planetary surface such as Mars or the Moon, were reduced gravity levels may lead to physiologic deconditioning similar to what is seen in microgravity. In particular, it may be found that human reproduction (gestation) requires 1g or near-Earth-normal gravity levels. If this is the case, then rotating habitats will find their place in the many regions of the cosmos that mankind sets off to explore.
ACKNOWLEDGEMENTS
The author wishes to recognize the financial support of this work by the Space Studies Institute and the administrative support by M.I.T.’s Man-Vehicle Laboratory.
REFERENCES
Bechler, B., Cogoli, A., & Mesland, D., Lymphocytes Are Sensative to Gravity (G). Natur Wissenschaften, 1986, 73, 400-403.
Bergman, S.A., Johnson, R.L., & Hoffler, G.W. Evaluation of the electromechanical properties of the cardiovascular system after prolonged weightlessness. In R.S. Johnston and L.F. Dietleing (Eds), Biomedical results from Skylab (NASA SP-377). Washington, D.C.: U.S. Government Printing Office, 1977.
Cogoli, A. Hematological and immunological changes during spacenight. Acta Astronautica, 1981, 8(9-10): 99S-1002.
Cogoli, A., Tschopp, A., Fuchs-Bislin, P., Cell Sensitivity to Gravity. Science, 1984, 22S (46S8), 228-230.
Donaldson, Charles L., Hutley, Stephen B, Vogel, John M, Hattner, Robet S., Bayers, J.H., and McMillan, D.G., Effect or Prolonged Bed Rest on Bone Mineral. Metabolism, vol. 19, no. 12, 1970, pp. 1071-1084.
Gazenko, 0 .0., Grigor’yev, A.I. & Natochin, Yu.V. Fluid-electrolyte homeostasis and weightlessness. From JPRS, USSR Report: Space Biology and Aerospace Medicine, 30 October, 1980, 14(5):1-11.
Gazenko, O.G., Il’in, Ye. A., Genin, A.M., Kotovskaya, A.R., Korol’kov, V.1., Tjigranyan, R.A., & Portugalov, V.V., Principal results of physiological experiments with mammals aboard the Cosmos 936 biosatellite. Space Biology and Aerospace Medicine, 1980, 14(2): 33-37.
Graybiel, A., Angular Velocities, Anautar Accelerations, and Coriolis Accelerations. Foundations of Space Biology and Medicine, Chapter 7, Volume II, Book One, Edited by Melvine Calvin and Oleg G. Gazenko, 197S, p. 247 -304.
Graybiel, A., Prevention or Motion Sickness In the Slow Rotation Room by Incremental Increases In Strength or Stimulus. Fifth Symposium on The Role of the Vestibular Organs in Space Exploration (Naval Aerospace Medical Institute, Pensacola, Florida). Office of Technology Utilization NASA. 1971.
Graybiel, A., Vestibular Mechanisms Underlying Certain Problems in a Rotating Spacecraft. Fifth Symposium on The Role of the Vestibular Organs in Space Exploration (Naval Aerospace Medical Institute, Pensacola, Florida). Office of Technology Utilization NASA. 1971. P. 3S – 39.
Graybiel, A., Clark, B., Zarriello, J., Observations on Human Subjects Living In a “Slow Rotation Room” for Periods or Two Days. A.M.A. Archives of Neurology, Vol.3, July 1960, P.55 – 73.
Graybiel, A., Kennedy, S., Knoblock, F., The Effects or Exposure to a Rotating Environment (10 RPM) on Four Aviators ror a Period of Twelve Days. Bureau of Medicine and Surgery, Project MR005, Subtask 1 Report No. 111, (NASA Order No. R-93), 30 March 196S.
Graybiel, A., Knepton, J., Direction-Specific Adaptation Effects Acquired in a Slow Rotation Room. Aerospace Medicine, 43(11), November 1972, P 1180 – 1189.
Graybiel, A., Miller, E.F., Homick, J.L., Experiment M131. Human Vestibular Function. Chapter 11, Biomedical Rcsu1ts of Skylab, NASA, Washington D.C., P. 74 – 90, 1977.
Graybiel, A., Wood, C., Rapid Vestibular Adaptation in a Rotating Environment by Means of Controlled Head Movements. Aerospace Medicine, 40(6), June 1969, P. 638 – 343.
Green, J.A., Peacock, J.L., Holm, A.P., A Study of Human Performance In A Rotating Environment. Research Repon # SD 7Q-456, conducted under contract no. NASl-9711 by North American Rockwell Corp., NASA CR 111866. 1971.
Guedry, F.E., Comparison or Vestibular Effects In Several Rotating Environments. First Symposium on The Role of the Vestibular Organs in Space Exploration (Naval Aerospace Medical Institute, Pensacola, Florida). Office of Technology Utilization NASA. 1965. P. 243-255.
Guedry, Fred, Visual Control or Habituation to Comples Vestibular Stimulation In Man, Acta oto-laryng, Vol S8, 1964.
Guedry, Fred, Habituation to Complex Vestibular Stimulation In Man: Transfer and Retention or Effects from Twelve Days or Rotation at 10 RPM, Perceptual and Motor Skills, 21, 196S, 459-481.
Jankovich, J.P., Lange, K.O., Structural Development or Bone in the Rat under Earth Gravity, Hypergravity, and Simulated Weightlessness. AIAA Paper No. 71-895 , AIAA/ASMA Weightlessness and Artificial Gravity Meeting, August 1971.
Johnson, R., Kirkendall, D., Psycholphysloloalc Responses to Rotary Motions. Res-Q-Am-Assoc Health-Phys-Educ. 41(4), 1970 December, P 489-49S.
Jones, G., Origin Significance and Amelioration or Coriolis Illusions from the Semicircular Canals: A Non-Mathematical Appraisal, Aerospace Medicine, 41(5), 1970 May, P 483 – 490.
Letko, W., Spady, A.A.Jr., Walking In Simulated Lunar Gravity. 4th Symposium on The Role of the Vestibular Organs in Space Exploration (Naval Aerospace Med Inst. Pensacola, Fl). Office of Tech Utilization, NASA. 1970, P. 347 – 351.
National Commission on Space, Final Report, Pioneering the Space Frontier, Bantam Books, 1986.
Nicogossian, A.E., Parker, J.F., Space Physiology and Medicine, NASA SP-447, Washington, D.C., U.S. Government Printing Office, 1982.
O’Laughlin, T. Brady, J., Newson, B., Reach Effectiveness In a Rotating Environment. Aerospace Medicine, 39 (S), 1968 May, P 505 – 508.
Oman, C.M ., A Heurlstlc Mathematical Model for the Dynamics of Sensory Confflct and Motion Sickness. Acta Otolaryng Suppl. 392
Oman, C.M., Lichtenberg, B.K., Money, K.E., McCoy, R.K., MIT/Canadian Vestibular Experiments on Spacelab-1: Space Motion Sickness: Symptoms, Stimuli, and Predictability. Exp. Brain Res., 1986.
Piland, W.M., Hausch, H.G., Maraman G.V., Deslan of Experimental Studies of Human Performance Under Influences of Simulated Artificial Gravity, Fifth Symposium on The Role of the Vestibular Organs in Space Exploration (Naval Aerospace Medical Institute, Pensacola, Florida). Office of Technology Utilization, NASA. 1971.
Ramsey, H., Human Factors and Artificial Gravity: A Review. Human-Factors, 13(6), 1971 December, (REVIEW) P 533 – 542.
Reason, J.T., Motion Sickness Adaptation a Neural Mismatch Model. J.R. Soc. Med, 71: 819-829.
Stone, R.W., Jr., An Overview of Artificial Gravity. Fifth Symposium on The Role of the Vestibular Organs in Space Exploration (Naval Aerospace Medical Institute, Pensacola, Florida). Office of Technology Utilization NASA. 1971.
Stone, R. W., and Letko, W., Effects of Rotation on the Ability of Subjects to Perform Simple Tasks. In: A Report on the Research and Technological Problems of Manned Rotating Spacecraft. NASA TN D-I504. Hampton, VA.: Langley Research Center, 1962. Pg 85-90.
Stone, R.W.,Jr., Piland, W.M. Potential Problems Related to Weightlessness and Artificial Gravity. NASA Technical Note D-4980, NASA, Washington, DC January 1969 P. 1-60.
Stone, R.W.,Jr., Piland, W.M., Letko, W., Certain Aspects of Onboard Centrifuges and Artificial Gravity. Fourth Symposium on The Role of the Vestibular Organs in Space Exploration (Naval Aerospace Medical Institute, Pensacola, Florida). Office of Technology Utilization NASA. 1970 P. 331-345.
Stupakov, G.P. Artificial gravity as a means of preventing atrophic skeletal changes, Space Biology and Aerospace Medicine, 1981, 1S(4):88-90.
Sulzman, F.M., NASA Report: Advanced Missions with Humans In Space, NASA Headquaters, January 8, 1987.
Thompson, A.B., Physiological Deslan Criteria for Artificial Gravity Environments In Manned Space Systems. Symposium on The Role of the Vestibular Organs in Space Exploration (Naval Aerospace Medical Institute, Pensacola, Florida). Office of Technology Utilization, NASA. SP-77, 196S.
Thornton, W. E., Hoffler, G. W., & Rummel, J.A. Anthropometic changes and fluid shifts. In R.W. Johnston and L.F. Dietleing (Eds), Biomedical results from Skylab (NASA SP-377), Washington D.C., 1977.
Thornton, W. E.,& Rummel, J.A. Muscular deconditioning and its preventation In Space flight. In R. S. W. Johnston and L.F. Dietleing (Eds), Biomedical results from Skylab (NASA SP-377), Washington D.C., 1977.
copyright Peter H. Diamandis, 1987
Space Manufacturing volume 6. The proceedings of the 1987 SSI Princeton Conference
